
Health Care Administration Wastes Half a Trillion Dollars Every Year



Health insurers are actually very bad.
Last week, an individual gunned down UnitedHealthcare CEO Bryan Thompson in the streets of Manhattan. The gunman wrote “deny,” “defend,” “depose” on the bullets he shot, suggesting that this killing was motivated by a dislike of UnitedHealthcare’s business practices, which are also the business practices of the private health insurance industry as a whole.
At the same time as that was going on, the American Society of Anesthesiologists, a lobbyist organization, criticized Blue Cross Blue Shield for declaring that it would curtail reimbursements for anesthesia care that goes beyond a certain level. This criticism generated a backlash that resulted in BCBS backing down from the policy.
The combination of these two events has jolted the US health care system back into the discourse in a way not seen since 2020, including many tweets and articles from prominent pundits like Matt Yglesias, Dylan Matthews, Noah Smith, and Eric Levitz. The quick consensus among these pundits is that dislike of the private insurers is overblown and that the main problem lies with providers and their overcharging ways. This conclusion relies upon several factual misunderstandings and very questionable analysis that I aim to correct below.
The Scourge of Administrative Costs
From a system design perspective, the main problem with our private health insurance system is that it is extremely wasteful. All health care systems require administration, which costs money, but a private multi-payer system requires massively more than other approaches, especially the single-payer system favored by the American left.
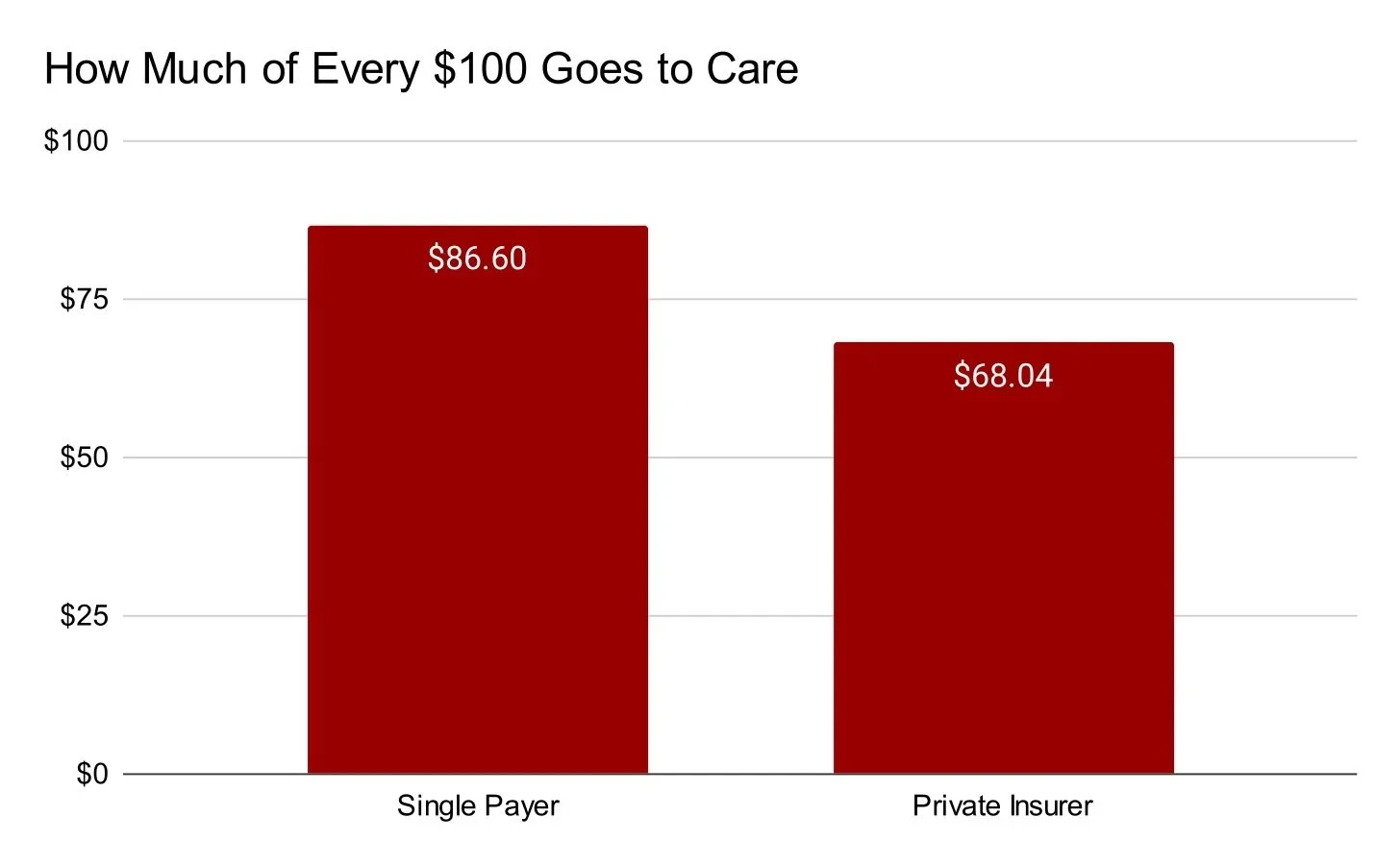
To get your head around why this is, think for a second about what happens to every $100 you give to a private insurance company. According to the most exhaustive study on this question in the US — the CBO single-payer study from 2020 — the first thing that happens is that $16 of those dollars are taken by the insurance company. From there, the insurer gives the remaining $84 to a hospital to reimburse them for services. That hospital then takes another $15.96 (19 percent of its revenue) for administration, meaning that only $68.04 of the original $100 actually goes to providing care.
In a single-payer system, the path of that $100 looks a lot different. Rather than take $16 for insurance administration, the public insurer would only take $1.60. And rather than take $15.96 of the remaining money for hospital administration, the hospital would only take $11.80 (12 percent of its revenue), meaning that $86.60 of the original $100 actually goes to providing care.
Put differently, private insurers currently have administrative costs that are 1,000 percent what they would be under single-payer while hospitals currently have administrative costs that are 158 percent what they would be under single-payer. The excess administrative expenses of both the payers and the providers are because of the multi-payer private health insurance system that we have.
When you add it all up, excess administrative expenses — defined as administrative expenses we have under the current system that we would not have under single-payer — are equal to 1.8 percent of GDP, or $528 billion per year.
Large numbers like that can be hard to understand, so I’ve prepared this chart below that compares the cost of excess health care administration to various other spending items:

In some ways, this chart is misleading because the spending on the other bars actually does something, whether fund important production or provide important income support. Excess health care administration does neither of those things. It’s just a total waste.
You know how often Republicans gesture vaguely towards the idea that the federal workforce is a do-nothing waste? While this claim doesn’t apply to the federal workforce, it is actually true of excess health care administration, which costs the country nearly twice what the entire federal workforce costs.
Imagine setting up an economic sector slightly larger in size than the entire public college sector but, rather than producing educational services for over 13 million students, it produced nothing except frustration and annoyance. That’s the extent and nature of excess health care administration in the US. It’s totally insane and waiving it off as a triviality is really misguided.
Provider Rates
One funny aspect of the recent discourse blip about provider payment rates is how at odds it is with the way things went the last time there was a public debate about the US health care system. During that period, ahead of the 2020 election, I was constantly having to fight with people and organizations who insisted that it would not be possible to cut provider payments as low as some single-payer proposals suggested. The argument from opponents was that doing so would result in some kind of mass exodus from and then collapse of the health care sector. Now, these rate cuts are being assumed as doable in order to argue that the ire directed at insurers is misdirected.